

Every 40 seconds a person dies of suicide somewhere in the world. Over 800 000 people die by suicide every year. Every suicide is a tragedy that affects families, communities and entire countries and has long-lasting effects on the people left behind.
The suicide occurred throughout the lifespan and was the second leading cause of death among 15–29-year-olds globally in 2016. Therefore, it has become a public health concern in developing countries such as those in Southeast Asia (SEA).
Cagande and Foo on the paper Suicide Among Southeast Asian Youth wrote in Southeast Asia, the suicide among youth has increased. There appear to be specific predisposing and risk factors, psychiatric diagnoses, and access to means of self-harm among youth who either thought of suicide, attempt suicide, or complete suicide in most of these countries
Based on 2016 data, in Southeast Asia, Thailand has the largest suicide ratio among ten countries, with the ratio 14.4 case for every 100.000 population, while male becomes the most suicide sex than female. The second country with the highest suicide rate is Singapore, followed by Laos. Meanwhile, Brunei Darussalam, Indonesia and Philippines are the countries with the lowest suicide ratio in the SEA.
Suicide Ration per 100.000 population in Southeast Asia Countries
| Country | Both Sexes | Male | Female |
| Thailand | 14.4 | 23.4 | 5.9 |
| Singapore | 9.9 | 13.8 | 6.1 |
| Laos | 8.6 | 11.4 | 5.7 |
| Myanmar | 7.8 | 5.9 | 9.5 |
| Viet Nam | 7.3 | 10.9 | 3.7 |
| Malaysia | 5.5 | 7.8 | 3.2 |
| Cambodia | 5.3 | 7.8 | 2.9 |
| Brunei | 4.6 | 6.4 | 2.7 |
| Indonesia | 3.4 | 4.8 | 2 |
| Philippines | 3.2 | 4.3 | 2 |
Source: WHO
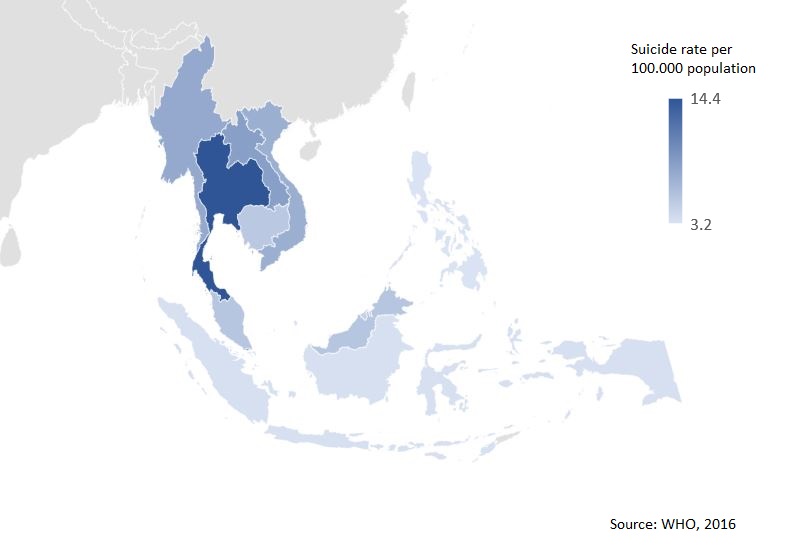
Suicide Rate in Southeast Asia (WHO, 2016)
World Health Organization (WHO) said around 79% of global suicides occur in low- and middle-income countries. It is estimated that about 20% of global suicides are due to pesticide self-poisoning, most of which occur in rural agricultural areas in low- and middle-income countries. Other common methods of suicide are hanging and firearms.
While the link between suicide and mental disorders (in particular, depression and alcohol use disorders) is well established in high-income countries, many suicides happen impulsively in moments of crisis with a breakdown in the ability to deal with life stresses, such as financial problems, a relationship break-up or chronic pain and illness.
Also, experiencing conflict, disaster, violence, abuse, or loss and a sense of isolation are strongly associated with suicidal behaviour. Suicide rates are also high amongst vulnerable groups who experience discrimination, such as refugees and migrants; indigenous peoples; lesbian, gay, bisexual, transgender, intersex (LGBTI) persons; and prisoners. By far the strongest risk factor for suicide is a previous suicide attempt.
Suicide is a complex issue, and therefore suicide prevention efforts require coordination and collaboration among multiple sectors of society, including the health sector and other sectors such as education, labour, agriculture, business, justice, law, defence, politics, and the media. These efforts must be comprehensive and integrated as no single approach alone can make an impact on an issue as complex as suicide.
WHO said there are several measures can be taken to prevent suicides, include:
- reducing access to the means of suicide (e.g. pesticides, firearms, certain medications);
- responsibly reporting by media;
- introducing alcohol policies to reduce the harmful use of alcohol;
- early identification, treatment and care of people with mental and substance use disorders, chronic pain and acute emotional distress;
- training of non-specialized health workers in the assessment and management of suicidal behaviour;
- follow-up care for people who attempted suicide and provision of community support.